Vasoconstriction and Vasodilation, via Effect Index
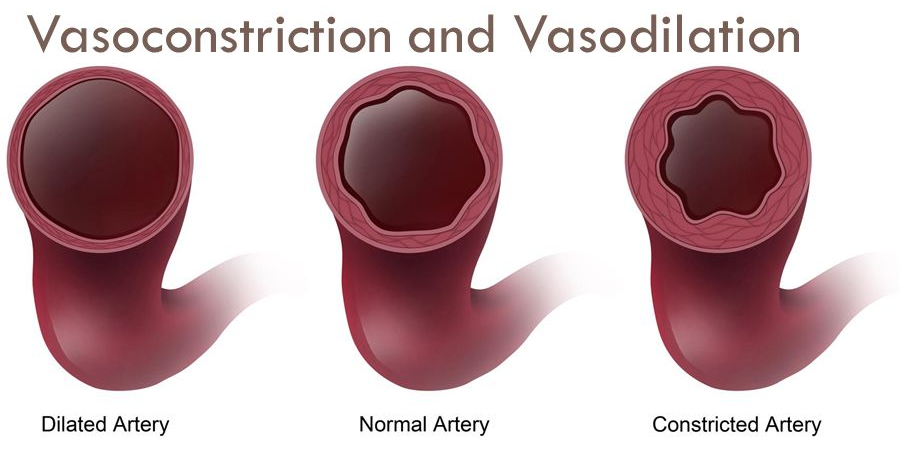
Vasoconstriction
A narrowing of blood vessels throughout the body that produces sensations of cold extremities, tingling in the fingers and toes, and a general feeling of circulatory restriction. Users may notice their hands and feet becoming pale, numb, or uncomfortably cold, sometimes accompanied by a sense of tightness in the chest or head.
Description
Vasoconstriction is experienced subjectively as a constellation of sensations related to reduced blood flow to the peripheral tissues. From a first-person perspective, the earliest signs are often cold fingers and toes that feel slightly numb or tingly, as if one has been sitting in a cold room. As the effect intensifies, the extremities may take on a pale or bluish tinge, and there can be an uncomfortable sense of pressure or tightness in the head, chest, or limbs. Some users describe a feeling of the body "clamping down" on itself, with muscles feeling harder and less supple than normal.
The severity of vasoconstriction follows a dose-dependent curve and varies significantly between substances. At mild levels, it may present as nothing more than slightly cool hands and a subtle sense of circulatory restriction that is easily ignored. At moderate levels, the hands and feet become noticeably cold and pale, cramping may occur in the extremities, and there can be an unpleasant headache from restricted cranial blood flow. At severe levels, vasoconstriction can become genuinely dangerous, with extremities turning white or blue, significant pain in the fingers and toes, and dangerously elevated blood pressure.
Vasoconstriction manifests in several distinct patterns depending on the substance and individual physiology. Peripheral vasoconstriction primarily affects the hands, feet, and skin, leading to cold extremities and pallor. Cerebral vasoconstriction affects blood vessels in the brain and can produce headaches, visual disturbances, and in rare cases, stroke-like symptoms. Coronary vasoconstriction affects the heart's blood supply and poses the most acute danger. Some substances produce predominantly one type over others.
The pharmacological mechanism involves activation of alpha-adrenergic receptors and serotonin receptors (particularly 5-HT2B and 5-HT1B) on vascular smooth muscle cells, causing them to contract and narrow the vessel lumen. Substances that release norepinephrine or act as direct alpha-agonists produce vasoconstriction through the sympathetic nervous system. Ergot-derived compounds and tryptamines have particular affinity for serotonin receptors on blood vessels, which explains their pronounced vasoconstrictive properties.
Vasoconstriction is particularly prominent with ergot-derived substances such as LSD and LSA (especially Hawaiian baby woodrose and morning glory seeds, which contain higher ratios of vasoconstrictive ergot alkaloids). Stimulants including cocaine, amphetamines, and synthetic cathinones produce significant vasoconstriction through catecholamine release. Many tryptamine psychedelics, NBOMe compounds, and DOx series phenethylamines also carry notable vasoconstrictive loads. Even caffeine produces mild vasoconstriction.
Safety considerations for vasoconstriction are significant. Severe vasoconstriction can lead to hypertensive crisis, particularly when combined with other vasoconstrictive substances or in individuals with pre-existing cardiovascular conditions. The combination of stimulants with ergot-derived psychedelics is particularly risky. Harm reduction measures include staying warm, gentle movement to promote circulation, and avoiding vasoconstrictive combinations. Substances like ibuprofen (a mild vasodilator) may provide some relief, though their use should be researched carefully. Any signs of severe vasoconstriction — white or blue extremities, chest pain, severe headache — warrant immediate medical attention.
Intensity Levels
Level 1 — Threshold
20%Slightly cool fingers and toes, barely noticeable. Mild sense of circulatory restriction if one pays attention.
Level 2 — Light
40%Noticeably cold extremities with mild tingling. Hands and feet feel slightly less sensitive. May want to put on warm clothing.
Level 3 — Moderate
60%Cold, pale extremities with numbness and tingling. Possible headache from restricted blood flow. Uncomfortable tightness in muscles and limbs.
Level 4 — Strong
80%Painful cold in extremities with visible pallor or blue tinge. Significant headache, possible cramping. Blood pressure notably elevated.
Level 5 — Overwhelming
100%Dangerous level of vascular restriction with white or cyanotic extremities, severe hypertension, intense headache, and risk of ischemic injury.
Safety & Danger Notes
Warning
Severe vasoconstriction can cause dangerously elevated blood pressure, ischemia (tissue damage from blood flow restriction), and in extreme cases, stroke or heart attack. Combining multiple vasoconstrictive substances dramatically increases risk. Individuals with cardiovascular conditions, Raynaud's disease, or hypertension are at elevated risk. Seek medical attention for white/blue extremities, chest pain, or severe persistent headache.